Sick Roses: Disease And The Art Of Medical Illustration
By Mark Dery


Kim Carsons, the “morbid youth of unwholesome proclivities” who stars in William S. Burroughs’s novel The Place of Dead Roads, would love Richard Barnett’s gorgeously illustrated new book, The Sick Rose: Disease and the Art of Medical Illustration. In his father’s “extensive and eclectic library,” Kim discovers a trove of medical texts, which he devours, driven by his “insatiable appetite for the extreme and sensational”:
He loved to read about diseases, rolling and savoring the names on his tongue: tabes dorsalis, Friedreich’s ataxia, climactic buboes…and the pictures! the poisonous pinks and greens and yellows and purples of skin diseases, rather like the objects in those Catholic stores that sell shrines and madonnas and crucifixes and religious pictures. There was one skin disease where the skin swells into a red wheal and you can write on it. It would be fun to find a boy with this disease and draw pricks all over him. Kim thought maybe he would study medicine and become a doctor, but while he liked diseases, he didn’t like sick people.
As a longtime habitué of medical museums and, less happily, an all-too-frequent visitor to the O.R. (short version: cancer, post-op complications), I know the types: the connoisseur of the Pathological Sublime, because I am one, and the misanthropic doctor who puts the irony in “caregiver,” because I’ve met him in the cancer ward.
Just what is it that makes some of us not only not avert our eyes but fasten onto images like the ones in Barnett’s book, antique medical illustrations taken from the collections of the Wellcome Library in London? In The Sick Rose, Barnett—a professor at Pembroke College, Cambridge who was well on his way to a degree in forensic pathology before he veered off into the humanities—has curated a collection of mostly 18th and 19th-century images of such gruesome beauty or revolting grossness they make the mind gasp. Here is a delicately, almost tenderly rendered sketch of a nude young woman with ichthyosis, her head discreetly cropped off, her girlish body disfigured by Rorschach-like blots. Here, on the book’s cover, is an unforgettable portrait of a young Viennese woman depicting her an hour after she contracted cholera—and a mere four hours before she died from it. There’s a weird aesthetic jolt, almost a ghastly beauty, to her glaucous skin and blue lips, the ironic contrast between her demure braided hairstyle and the high-opera melodrama of her horrified expression. Here is an old man with leprosy, his face a mass of crusted growths that look uncannily like crumbling rock, which makes you think of The Thing from The Fantastic Four, then makes you feel cheap and ugly for doing so, because there was a human being in there, behind the grotesque mask the disease made him wear, beneath the pain the disease—and the people who shrank from his touch—made him feel. Here, too, is a woman with dermatographic urticaria, the skin condition Kim dreamed of putting to amusing use; true to Kim’s fantasies, someone—a doctor?—has used a needle or a pencil to write on her skin, causing the words to stand out in welts, like the writing on the possessed girl’s belly in The Exorcist.

Barnett is a careful, erudite historian of science, not to mention a fine stylist who turns a nice phrase, but what makes The Sick Rose so affecting is his refusal to deny the perverse pleasures of this stuff—the “extreme and sensational” material that captivates the Kim Carsons in some of us—while at the same time forcing us to confront the politics of looking; the psychological and philosophical costs of savoring the pain of others, pain that reverberates down through the centuries in images that once seen, can’t be unseen.
Mark Dery: I imagine the young Richard Barnett as the sort of child who would stare, in undisguised fascination, at some abject sufferer with an enormous goiter, and who grew into the kind of teenaged boy who kept under his mattress, in place of the usual Playboy, a color atlas of pathological anatomy. Am I wrong?

Richard Barnett: Quite wrong. I was an unusually shy and introverted child (perhaps it’s more accurate to say a typically shy and introverted English child), with a positive horror of deformity, violence, and viscera. Skulls especially, for some reason: I recall being utterly spooked for some weeks by the sight of a sheep’s skull we found out on a walk when I was perhaps seven or eight. (I wonder if I’d caught sight of a Dennis Wheatley paperback somewhere beforehand?) The bareness of the teeth, the emptiness of the eye-sockets, the sense of something ghastly lurking beneath the surface of life—as Eliot says, “the skull beneath the skin.” So there was a kind of fascination, certainly, but it was something I could only bear to glimpse out of the corner of my eye, something I couldn’t confront directly until I was much older. I was far happier hidden away with The Book of a Thousand Poems.
M.D.: Looking back, was there any incident or ongoing obsession, in your childhood, that now seems premonitory of the interests that flowered in The Sick Rose?
M.D.: A few. One quite out of my control: throughout my life I’ve had quite a bit of surgery, usually an operation every six or seven years or so. (I’m not seriously ill, thank heavens; just not very well put together.) As a boy this, quite naturally, scared the hell out of me: the pain, of course, but perhaps more the sense of losing control over one’s body, of being naked and vulnerable under the gaze of impassive strangers, and the feeling of being abandoned to one’s surgical fate by one’s parents, helpless as they are in that situation.

As an adult I’ve come to feel very different: going under with a general anesthetic is one of the great metaphysical experiences, and one I think everyone should experience once. Another was reading, at the age of eight or nine, Keith Simpson’s Forty Years of Murder. Simpson was one of the leading British forensic pathologists (I think you call them medical examiners) in the mid-20th century, and reading his autobiography set me on my early career path to medical school. Oddly enough it wasn’t the gory aspects of his work that fascinated me, but rather the narrative, almost imaginative side: the reconstruction of a story, a scene, perhaps an identity, from scattered and fragmentary clues, exactly what I now do as a historian.
M.D.: In your introduction, you talk about the cognitive dissonance inspired by antique medical illustration. Looking at this stuff crosses our signals; our intellects say aesthetic rapture, our emotions say visceral horror. A good deal of it is exquisitely rendered, with obvious artistic intent; in a lot of these illustrations, the aesthetic eye and the scientific gaze share equal billing. At the same time, much of the subject matter is pretty grisly stuff: dissections, disfiguring skin diseases, the ravages of cancer, ulcerations caused by typhoid, the prematurely wizened face of an infant afflicted by hereditary syphilis.
To what extent do you experience these sorts of conflicted feelings, when looking at medical illustrations like the ones you’ve collected in The Sick Rose? How big a part of the motivation behind the book was the desire to make sense of the uncanny power of these images; to parse the feelings they evoke?
R.B.: I think something would be wrong if these illustrations did not evoke feelings of conflict and unheimlichkeitin us. One of the most difficult, and at the same time most rewarding, ways to engage with these images is to experience and reflect on the kinds of power they possess: sympathy, disgust, beauty, photo-realism, dignity, pity. I can’t do better here than to repeat what I wrote in the introduction: “[These images] give us, so to speak, the outside of the inside; they are insistently concerned with surfaces, but surfaces that in life and health are never seen … They present an uncanny spectacle of the dead body articulated: not only prepared and mounted for display, but also made to speak (in a voice that is not wholly its own).” There’s a peculiar and intimate kind of sublimity about them; they undermine the seeming integrity of the viewer’s own body by foreshadowing its ultimate destruction through disease, injury and death.

As I wrote the book, and spent more and more time with these depictions of suffering and disfigurement, I found myself becoming uneasy in ways I couldn’t pin down. It wasn’t until the book was finished that I could put this into words, in an essay for the Wellcome Library blog. Without repeating too much of that here, I found myself asking whether these images actually represent a form of human remains. And that makes me want to be very, very careful about what I do with them.
M.D.: Even so, you acknowledge that the anatomical and pathological textbooks and atlases created between the French Revolution and World War I—the “golden age of medical image-making,” in your estimation—constitute “a corpus of art that is beautiful and morbid, singular and sublime.” Reflecting on the aesthetic seductiveness and visceral repulsion of antique medical illustrations, you ask, “How should we understand this tension between ‘the beauty of the coats of the stomach’ and ‘the sight of a dead and mangled body’? Should we seek to resolve…it, or should we practice what…the medical student-turned-poet John Keats called negative capability—the capacity to be ‘in uncertainties, mysteries, doubts, without any irritable reaching after fact and reason’?”
In The Sick Rose, you leave the question hanging in the air. I’d be curious to hear you expand on it, if not resolve it.
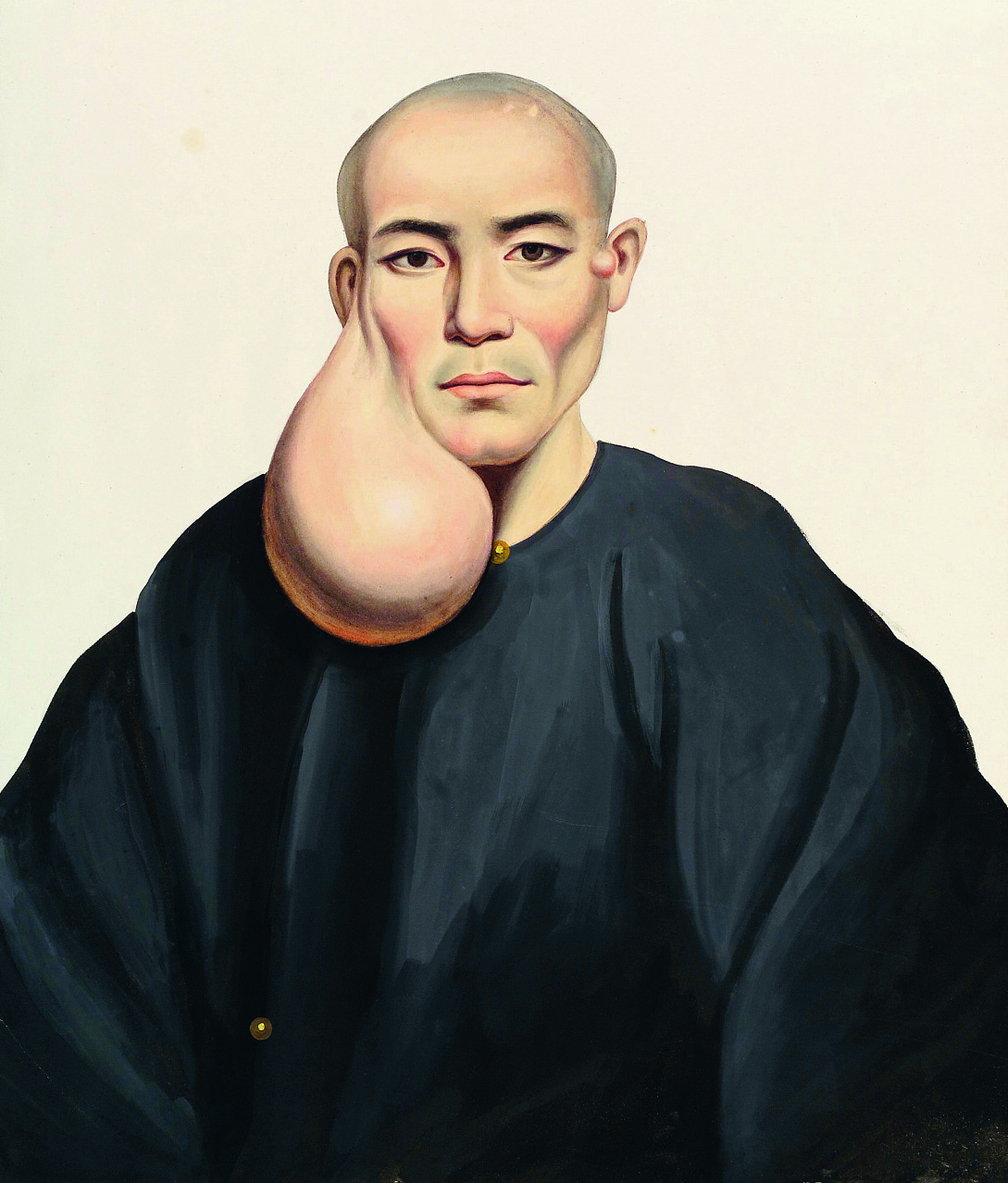
To prime the pump, I’ll say that I’ve always felt that the appeal (to some of us, at least!) of, say, wax moulages of diseases or deformities, or the 19th-century Chinese painter Lam Qua’s portraits of patients with grotesque tumors, owes something to our tendency, after Surrealism, to see such things as dreams made flesh. Also, the emotional and intellectual effect of this sort of thing is synonymous, in my mind, with the tug-of-war between wonder and terror that the 18th-century philosopher Edmund Burke calls the sublime. In fact, Oliver Wendell Holmes, Sr., in a brief, unsigned review of an exhibition of Lam Qua’s paintings (“Illustrations of Tumors among the Chinese,” Boston Medical and Surgical Journal, May 21, 1845), calls Qua’s visions of “monstrous diseased growths” an example of “the pathological sublime.”
R.B.: Well, it’s very Keatsian to leave the question hanging, and my own view is precisely that we should. I’d hate to resolve this tension, as it’s so fascinating, so thought-provoking. It’s not that I think these images should provoke a certain set of reactions, but rather that we should approach them in a way that acknowledges the power they have, and the roots of this power in our own fragile human condition. An earlier generation responded to this power by locking these images away (literally in some cases), and the current generation responds, in so many instances, by reframing these images as death kitsch or gross porn. Both attitudes, of course, reflect shifting cultural conditions, but both strike me as deeply inadequate. They dodge the central question of power, and neither helps to draw out the richness and depth these images embody (a word I found myself using far too often in successive drafts of the book) and the complexity of the responses they provoke.
Speaking of which: you’re absolutely right with regard to Surrealism. The uncanniness of these images resides in the fact that, like Dali and Magritte (and, of course, Bosch before them), they use the techniques and spaces of realist art to depict things that seem perverse, nightmarish, unreal.
M.D.: In a sense, Surrealism was born in the O.R. (or, if you like, the dissecting table): André Breton, the movement’s founder, studied medicine. The Surrealists drew inspiration from Lautréamont’s Maldoror, a bizarre, hallucinatory 19th-century novel whose best-known line, “Beautiful as the chance meeting, on a dissecting table, of a sewing machine and an umbrella,” became a Surrealist slogan. The Surrealist mechanism, par excellence, for forcing dreamlike free-association was a parlor game called “the exquisite corpse,” which involved creating Frankenstein-ian mash-ups of drawings or poetry. The Surrealist movie Un Chien Andalou, by Dali and Luis Buñuel, opens with a razor slicing into an eye with clinical dispassion. And, of course, Surrealism’s fundamental intent was to peel back our conscious defenses, exposing the innards of ourselves—to anatomize the unconscious.
More recently, iconoclastic novelists such as William S. Burroughs and J.G. Ballard have drawn inspiration both from Surrealism (the collage technique, “found” literature) and medicine: Burroughs, who briefly studied medicine, cut up and sutured texts together; one of his best-known literary alter egos is the drug-addled, hilariously depraved Dr. Benway. Ballard studied medicine at King’s College, with the intent of becoming a psychiatrist, and spoke often about the influence of medical imagery, specifically the experience of anatomizing a cadaver, on his literary imagination.
What do you make of the apparent connection, here, between the radical artistic imagination and medicine as transgression, directing our attention to disease, internal organs, and other aspects of the body society would rather not look at?

R.B.: The magnificent Dr. Benway has been in my thoughts a great deal over the past decade, as I dropped out of medical school, and searched for a frame in which to place my own questions about medicine and its power, and underwent more surgery, and tried to begin thinking with my whole body rather than just my brain. The flesh, and more specifically a sense of rage and frustration at its limitations, is the clue with which we are so often forced to begin our investigations, clinical and literary. For me, the telling term is autopsy, from a Greek root meaning to see for oneself, but also, surely, to see oneself. The body in the library is usually our own, and it’s no coincidence that culture and art are suffused with corporeal metaphors. “O, that this too too solid flesh would melt, thaw, and resolve itself into a dew,” and so on to your examples. One could write an entire thesis on your question, but it seems to me that the hidden link here is the libelous, barbarous, thrilling observation that a human being is a couple of hundred pounds of meat gifted with the troubling power to walk and talk and know something of itself.
M.D.:In the book, you ask, “What aesthetic and cultural values were inscribed in these images, and by whom?” It’s easy to detect social Darwinist ideas about race in Victorian medical imagery or the Romantic aesthetic in 19th-century depictions of tuberculosis sufferers. We applaud ourselves for questioning the purportedly “objective clinical gaze,” as you call it, of pre-modern medical imagery.
By contrast, it’s difficult to discern the cultural biases, ideological subtexts, and aesthetic influences in the medical imagery of our moment, brought to us by X-rays, CAT and PET scans, MRIs, ultrasound, and the like. Is that because such machine-made images truly are more representationally true, less prone to cultural and historical assumptions, than images created by the human hand? Or are we as blind to their aesthetic and ideological biases as, say, the Victorians were to the medical imagery of their day?
R.B.: This is a tricky one. As you say, we tend to regard the technologies of “mechanical objectivity” as simply better, more neutral, more true. But as a cultural historian I’m professionally suspicious of any sweeping claims to greater neutrality or objectivity. I’d say the most important thing to bear in mind about any kind of representation of the human body is that it is a representation and not the thing itself.
X-rays, for example, are just about the most widespread form of mechanical objectivity in modern medicine; they’re based on a technology—photography–which has been in common use for more than a century, and they certainly don’t look like an obvious instantiation of cultural values. But have you ever tried to interpret a simple standard chest X-ray? It’s an art. It requires a honed, experienced gaze which can’t (at least hasn’t yet) been reduced to a set of algorithms. It shows some things, particularly bones, in crisp detail, and others– soft tissues–in hazy, indistinct outline. It’s like anatomizing a cloud, or a ghost. The human element, the cultural and aesthetic and individual element, is still present and crucial.
Objectivity in science is always and everywhere a communal business, a matter of debating and agreeing on shared standards of rigor and interpretation, and enforcing these standards in the community of practitioners. So although it may be more difficult to see aesthetic and ideological undercurrents in these technologies, I think we can see them in the shifting styles and meanings of objectivity over the past couple of centuries. The grand claims made with regard to fMRI studies of the brain are a superb example of this. But don’t get me started on neuromania, cultural, scientific and educational, or we’ll be here until Christmas.

M.D.:You talk about the politics of “regarding the pain of others,” as Sontag put it—the dangers of commodifying or even just emotionally exploiting, for prurient purposes, images of disease, disfigurement, death. You wonder if such images “actually represent a form of human remains,” and urge us to think twice about the politics of looking, and to be “very, very careful” what we do with these images of other peoples’ pain.
In that light, I can’t help wondering what you think about the burgeoning interest, among erudite weirdoes and hipsters of the morbid persuasion, in the more obscure and curious corners of medical history. I’m thinking of the subcultural demographic attracted to the Morbid Anatomy Museum in Brooklyn, the reality-TV show Oddities, the Mutter Museum in Philadelphia, and of course books like yours. (Should we mention Gunther von Hagens’s Body Worlds exhibitions of “plastinated” cadavers? Arguably, they represent a crass, mass-market version of this traffic in “dark” medical imagery, reviving the public anatomy lessons of 17th-century Bologna for the age of Miley Cyrus and anal bleaching. And where does the fad for taxidermy fit into this phenomenon, if it does?) This emerging interest expresses itself primarily through the consumption of images.
R.B.: Tempting as it is to take a radical left turn into the negative dialectics of anal bleaching, I’ll say, first, that it’s absolutely not my place to tell anyone how they should respond to these images. Of course I’ll say to anyone who’ll listen that we should treat them with dignity, that we should take the time to appreciate the rich and complex themes they embody. I’m enormously hostile to those who grab clinical or historical images out of context and scatter them across Twitter or Pinterest with no purpose beyond lurid gawping.
But sick chic has many faces, and I find things like Morbid Anatomy and Oddities thoroughly heartening. (Full disclosure: I was scholar in residence at the Morbid Anatomy Library in April 2014; while I was there I got to know Evan Michelson and Mike Zohn of Oddities, and I’m now an honorary founding member of the Morbid Anatomy Museum.) Morbid Anatomy in particular has pioneered a way of opening these kinds of collections up to smart, curious, unorthodox folk outside the traditional confines of an academic museum or library, and long may it prosper. And I’m sympathetic to von Hagens, odd character though he may be. Plastination is streets ahead of old-fashioned formalin as a technique for preserving anatomical specimens, with enormous potential as a teaching tool in medical schools. It seems to me that what unites von Hagens and William Burroughs (apart from a taste for natty headgear) and all the individuals we’ve discussed here is an obsession with the old philosophical imperative: nosce te ipsum, “know thyself.” ![]()

All images via The Sick Rose: Disease and the Art of Medical Illustration by Richard Barnett, published by Thames & Hudson.




